

Dr Bart Post is a neurologist at Radboudumc hospital in Nijmegen, the Netherlands, specialising in Young Onset Parkinson’s. He leads an innovative care programme specifically aimed at young patients and their unique needs.
In an interview with Anne-Marie Demoucelle, he shares his expertise and provides valuable insights for patients, informal carers and caregivers.
——
***What exactly do we mean by Young Onset Parkinson’s?
For scientific purposes, we have agreed within the Movement Disorder Society that anyone under the age of 50 with Parkinson’s is classified as “young onset”. Under 21, we speak of juvenile Parkinson’s.
The disease manifests really differently in young people compared to older patients. For instance, in young onset we see genetic causes more often; under 50 years of age this is the case in about 20% of cases, but under 30 years of age it is even 30%. Disease progression also differs: in young people, the disease progresses more slowly, but they develop issues with medication more quickly. If you are under 40, almost everyone gets fluctuations in drug effectiveness and overexertion within five years, while in older people this occurs in only a third. In addition, we see dystonia – cramps in arms and legs – much more often in young patients, about 20% compared to only a few percent in older patients.
![]()
***What else makes Young Onset Parkinson’s different?
The impact on life is much broader. Young patients are still in the middle of their careers, often have young children or may want to start a family. The disease affects so many aspects of their lives: work, family, friendships, future plans. With young women, there are also specific questions about the menstrual cycle, pregnancy and hormones. So doctors are posed very different questions compared to older patients.
***What do we know about the causes of Parkinson’s in young people?
I always think of it as a ‘cake’ of causes. In young people, about 20-30% of the cake is genetic – sometimes one specific gene, but more often a combination of small genetic variations that make someone vulnerable. Another part, about a third, are environmental factors such as pesticide exposure, as well as protective factors such as caffeine consumption and exercise. And perhaps a third of the cake is still a big question mark – that’s where we simply don’t know what contributes to the onset of the disease.
***What about the heritability of Parkinson’s in young patients?
In mono-genetic forms, where one specific gene causes the disease, we can indeed say something about the likelihood of children inheriting it. But in most patients, even young ones, it involves a complex combination of factors. And this genetic complexity makes it difficult to provide good information without causing people unnecessary anxiety.
Take for instance the LRRK2 gene or the GBA gene. With both, you have a 50% chance of passing it on to your child. But if your child inherits the gene, with GBA only 20-30% actually get sick, and with LRRK2 about 30-40%. So apparently something else has to happen before someone develops symptoms.
***How does medication differ in young patients?
The main difference is that in young people the fluctuations in the effect of the drug levodopa and the overactivity occur much faster, often within five years. As a result, you have to more quickly add all kinds of drugs to keep the situation stable. You also see young patients opting much earlier for advanced treatment such as deep brain stimulation (DBS) or a drug pump. Sometimes as early as within four or five years, whereas in older patients this usually takes much longer.
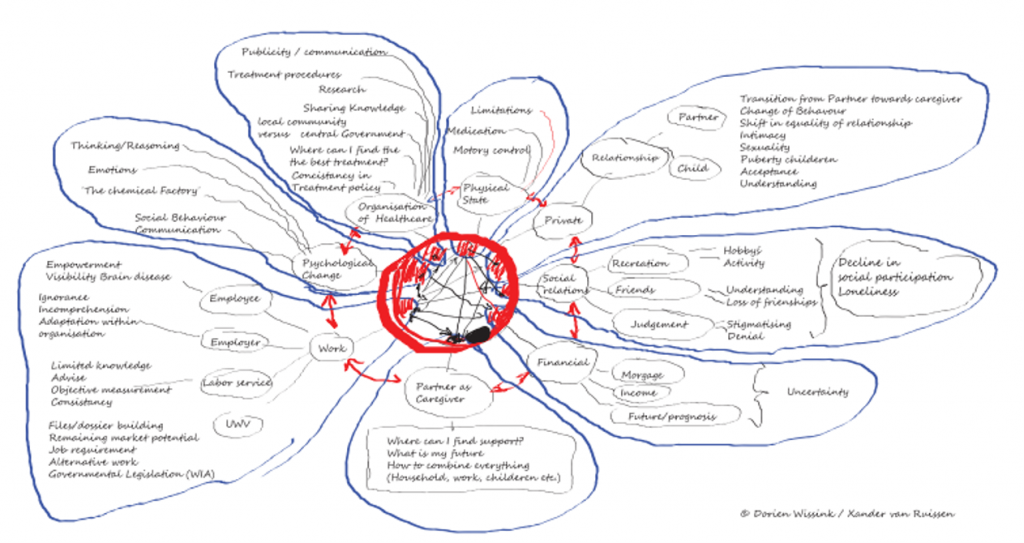 ***You work with a “mind map” approach. What does that entail?
***You work with a “mind map” approach. What does that entail?
One of my patients, Xander, once made a mindmap of the impact Parkinson’s had on his life. He showed me that what I was worried about as a doctor – motor skills, tremor, medication – was only a small part of his daily challenges.
The biggest impact came from issues around work, finances, relationships, children, future anxiety and stress. That opened my eyes and led to our programme for young Parkinson’s patients, in which we consider more than just motor symptoms. I have my own clinic for young people, but we also have a women’s clinic, a dystonia clinic, a genetics clinic, etc. all linked to those young people.
We encourage patients to make their own mind map. Show it to your neurologist and start talking about the many ways (Parkinson’s) impacts you. Sometimes that particular neurologist may not be able to do much to help you, but an expert elsewhere may be able to assist with your specific problem. So, start the conversation and don’t limit it to” “I have a tremor, here are some pills, until next time”.
***What can patients themselves do to improve their situation?
There are three things that always help, not just young Parkinson’s patients. First, exercise, preferably three times a week. We know that this has symptomatic effects and may even affect the progression of the disease. Secondly, nutrition is important, especially to properly align medication and diet. And third, stress management is crucial. Stress makes tremors and other symptoms worse. Learn to recognise stress and apply what works for you: mindfulness, yoga or other techniques. There is evidence that it not only reduces symptoms, but may even affect the course of the disease.
***What can you say more specifically about juvenile Parkinson’s patients?
Juvenile Parkinson’s is actually a very different condition from Young Onset Parkinson’s. In juvenile Parkinson’s, we see a hodgepodge of particular causes. For example, Huntington’s disease, when it presents in childhood, can look like Parkinson’s. There are many more rare syndromes among them that present similar symptoms.
So my advice is: if you have a child under 21 with Parkinson’s-like symptoms, always send him or her to a super-specialised centre. Extensive research should be done there to find the underlying cause, as there can be many rare conditions behind it. And the diagnosis makes a huge difference to treatment.
***What is your advice to family carers of young Parkinson’s patients?
My main advice is: don’t bury your head in the sand. If your partner gets Parkinson’s at a young age, it can also affect your life – the choices you make, the energy you have for your career or friends. Be open about it, engage in conversation, get help or seek support. Don’t struggle on your own.
The same applies to children of young Parkinson’s patients. We have people on our team who themselves grew up with a parent who developed Parkinson’s at the age of 30 or 40. They tell us that they had a different childhood, learned a lot, but also missed out on things that are part of a carefree childhood. If you experience that, seek help.
***Finally, what is your main message for young Parkinson’s patients?
I would say two things: first, if you get Parkinson’s at a young age, it is really different than if you are affected later. The disease behaves differently in young people, and therefore requires a different approach. And fortunately, there is more and more tailored expertise available. And secondly: make your own mind map. Understand how Parkinson’s affects your life and map that out. Because that really helps you and your carers to provide the right support.